How Cardiology Practices Can Improve Coding Accuracy
Last updated: July 14, 2026
Key Takeaways
Cardiology practices face 11.8% average claim denial rates. Documentation errors, not clinical mistakes, drive most of the revenue loss, estimated at $250,000-$400,000 annually for a $5M practice.
Common coding pitfalls include prior authorization gaps, modifier misuse, and weak medical necessity language. Payers catch these through automated edits, clinical review, and post-payment audits.
CIED and RPM billing (CPT 93298, 93299, 99454, 99457) requires precise documentation of device data, transmission thresholds, time logs, and provider signatures to meet 2026 payer and CMS requirements.
Monthly audits, cardiology-specific EHR templates, and real-time KPI tracking of first-pass acceptance rates can cut denials by up to 70% and improve revenue capture without adding staff.
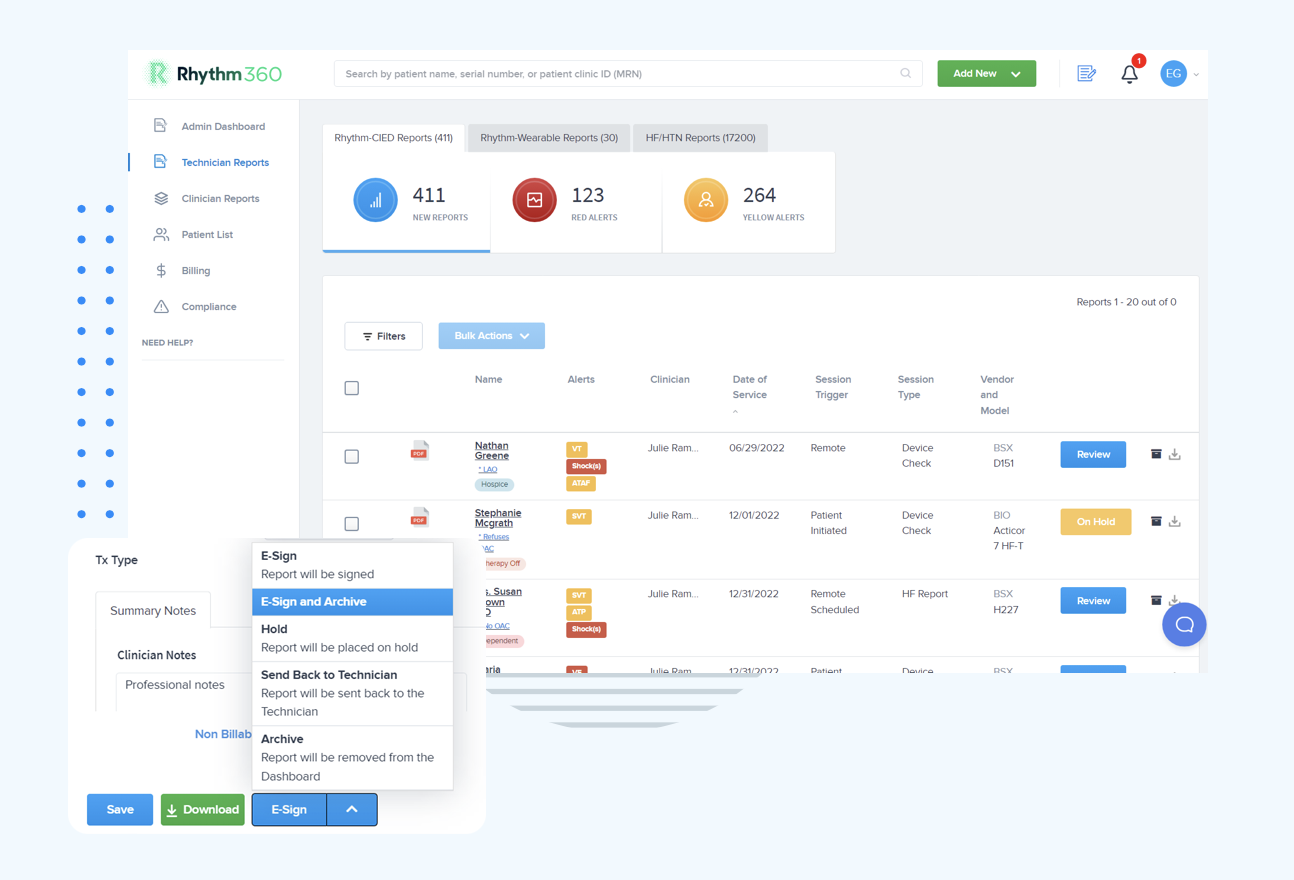
Rhythm360 consolidates CIED and RPM data into a single vendor-neutral platform that auto-populates audit-ready notes and flags compliance gaps. Schedule a demo to see how it strengthens your 2026 cardiology documentation and billing accuracy.
1. Prior Authorization and Modifier Errors Drive Most Denials
Prior authorization issues are a leading cause of cardiology denials. Cardiology claims are denied at overall rates of 15-25%, with medical necessity as the leading reason, often due to thin clinical documentation. Modifier errors rank as the second most common cause.
A pre-procedure documentation checklist prevents most of these denials. Every cardiology procedure note needs:
Patient symptoms and functional class (NYHA for heart failure, CCS for angina)
Relevant diagnostic findings with dates
Prior treatment history and response
A clinical rationale matching the payer's LCD criteria language
Provider signature with credentials and authentication date
Procedure example: Billing CPT 93452 (left heart cath only) instead of 93458 (left heart cath with coronary angiography) when both were performed can cost the practice lost Medicare reimbursement per case.
Pro Tip: Copy-forward documentation produces inconsistent symptom descriptions and contradictory plans that auditors treat as a compliance risk. Require clinicians to update each note field actively instead of carrying forward prior entries.
2. What CIED and RPM Claims Need to Survive Payer Review
These coding basics matter most when claims reach payer review, since CIED remote monitoring documentation faces a layered process: automated claim edits, clinical medical review, and post-payment audit. Payers compare diagnosis and procedure codes first, then review symptoms and decision-making, then examine utilization patterns in post-payment audits.
For CPT 99454, required enrollment artifacts include:
A physician order with documented medical necessity
Written patient consent with cost-sharing acknowledgment and date
ICD-10 diagnosis codes tied to the qualifying condition
Device type and provisioning record confirming FDA clearance
Proof of an established patient via an initiating visit
Pro Tip: Before submitting any RPM claim, verify four readiness gates: data volume (16+ transmitted days), time threshold (20+ minutes), a live two-way interaction, and confirmation the billing provider is not in a surgical global period.
Apply Modifier 26 on professional-component claims when the cardiologist interprets but does not own the equipment. Getting this wrong is one of the most common drivers of the denial gap above.
Building on that, use Modifier 59 (or XU) only when documentation explicitly supports a distinct service, never as a default.
Append vessel-specific modifiers (LC, LD, LM, RC, RI) on every PCI line item for commercial payers.
Rhythm360 in Action: Fragmented OEM portals force staff to manually reconcile transmission data across separate Medtronic, Boston Scientific, Abbott, and Biotronik logins before a single note can be written. Rhythm360 consolidates all CIED and RPM data into one vendor-neutral dashboard. It auto-populates audit-ready documentation with timestamped transmissions and CPT-compliant note fields, without adding headcount. As the University of Chicago Medicine reported after implementation: "We have improved billing and accountability for our patients after the integration."
Pro Tip: Direct integration between clinical documentation and billing systems pre-populates CPT codes, ICD-10 diagnoses, and provider credentials from the clinical record, eliminating manual transcription errors.
20+ minutes of clinical staff time, interactive communication record, date/duration/activity log
Integrated time-logging tool with activity descriptions; communication hub with Twilio call logs and audit trail
20 minutes per calendar month
Rhythm360 in Action:Staffing was always an issue for device clinics, which struggled with technician turnover and timely weekend coverage. Rhythm360's automated reporting and centralized dashboard reduce reliance on a single "super-user," so documentation continues regardless of staffing gaps. The platform achieves greater than 99.9% data transmissibility through redundant data feeds, computer vision, and AI-powered extrapolation, keeping transmission-day counts accurate and defensible at audit.
6. What the 2026 Code Updates Mean for Your Templates
Several 2026 code changes carry direct implications for cardiology documentation workflows.
For RPM billing, effective January 1, 2026, new CPT code 99445 covers 2 to 15 days of RPM data collection within 30 days, enabling billing for shorter monitoring windows that were previously unreimbursable, while revised CPT code 99454 applies specifically to 16 to 30 days of device data transmission.
Each update above requires a specific documentation fix. Here is what to change in your templates now:
Document ejection fraction values on all heart failure notes to support the new ICD-10-CM specificity requirements
Verify septal/interventricular placement language for the new conduction system pacing lead codes
Confirm AUC consultation documentation using G-codes (G1000-G1015) for advanced cardiac imaging claims
Pro Tip: The 2026 ICD-10-CM updates take effect October 1, 2025. Claims for services through September 30, 2026, must use the prior code set with no grace period. Build a hard cutover date into your EHR template update schedule.
Rhythm360 in Action:"That was a big piece for us, to have an integrated review of data from trained personnel." Rhythm360's optional 24/7/365 oversight by certified cardiac technicians, supervised by physicians, captures new 2026 code-specific documentation requirements, including device type, anatomic placement, and ejection fraction, at the point of clinical review rather than reconstructing them retroactively at billing.
As noted earlier, weak front-end controls can push first-pass denial rates to 15-20%, well above the 5-8% industry benchmark. Tracking specific KPIs at the CPT code level is how practices close that gap, not just watching the aggregate denial rate.
First-pass acceptance KPIs to monitor monthly for CIED and RPM services:
First-pass acceptance rate by CPT code (93298, 93299, 99454, 99457)
Transmission-day compliance rate: percentage of enrolled patients meeting the 16-day threshold
Interactive communication documentation rate for CPT 99457
Average days to denial resolution by denial reason code
Percentage of notes with complete provider authentication before claim submission
Practices using integrated device data and automated documentation workflows typically see an 80% reduction in critical-alert response time and up to 300% revenue lift through improved first-pass acceptance. Other platforms in the cardiac monitoring space exist. Rhythm360 focuses specifically on unifying CIED and RPM data capture, automated CPT-compliant documentation, and bi-directional EHR integration into a single vendor-neutral platform built for cardiology billing compliance.
Rhythm360 in Action: Rhythm360's administrative dashboard provides a real-time overview of patient compliance, critical alerts, and captured versus potential revenue based on CPT code requirements. This gives practice administrators the KPI visibility to act before a billing period closes rather than after a denial arrives.
What documentation supports CPT codes 93298 and 93299 for CIED remote monitoring?
CPT 93298 covers remote interrogation device evaluation for a CIED with physician analysis, review, and report. The note must document the device type, manufacturer, model, and serial number, the transmission date and method, interrogation findings including sensing thresholds, pacing thresholds, lead impedance, and battery status, a complete arrhythmia episode log with dates, durations, and ventricular rates, a clinical interpretation of findings, and the reviewing provider's signature with credentials. CPT 93299 covers the physician's interpretation and report component and requires a separately authenticated signed report. Unsigned or improperly authenticated notes invalidate claims even when all clinical content is present. Platforms that auto-populate structured reports from normalized OEM data and route them to a clinician review queue with one-click authentication eliminate the most common denial triggers for these codes.
Which 2026 changes affect CIED and heart failure billing most?
Three 2026 changes carry the highest impact. First, ICD-10-CM code I50.9 stays valid and unchanged for heart failure, unspecified, with guidance to use more specific I50 codes when documentation allows. Under the 2026 CMS-HCC V28 model, reduced-EF and preserved-EF heart failure codes map to the same HCC 226 with no payment difference, so ejection fraction values must appear in every heart failure note. Second, new ICD-10-PCS codes effective April 1, 2026 require explicit documentation of device type, anatomic placement, and approach for conduction system pacing lead insertions, and that documentation must exist in the operative note rather than get reconstructed at billing. Third, revised CPT code 99454 now applies specifically to 16 to 30 days of device data transmission, and new CPT code 99445 covers 2 to 15 days, enabling billing for shorter monitoring windows that were previously unreimbursable. Practices must update EHR templates and billing workflows to reflect both the October 1, 2025 ICD-10-CM cutover and the January 1 CPT changes, with no grace period on either.
How can a practice reduce RPM denials without hiring more staff?
Documentation that fails to meet CMS threshold requirements at billing time, not clinical errors, drives most RPM denials. The most effective fix is automating documentation capture so transmission-day counts, time logs, and interactive communication records get generated at the point of service instead of assembled retroactively. Practices should use a platform that monitors each enrolled patient's transmission-day count in real time and alerts staff before the billing month ends when a patient risks falling below the 16-day threshold. Time entries for CPT 99457 must include the specific date, duration in minutes, and a detailed description of qualifying clinical activities, not summary entries. Enrollment artifacts including the physician order, patient consent, and ICD-10 diagnosis codes must stay stored and retrievable by the billing team. When these elements are automated and centralized, practices maintain audit-ready documentation across a large CIED and RPM population without adding headcount proportionally.
What is the financial impact of improving first-pass acceptance rates?
As noted earlier, this documentation gap can cost a $5M practice $250,000-$400,000 annually in recoverable revenue. Closing the denial-rate gap through structured templates, monthly audits, and automated documentation workflows produces measurable revenue recovery. For CIED and RPM services specifically, the impact compounds because denials on codes like 93298, 93299, and 99454 are often systemic. The same documentation gap affects every claim in a billing period. Integrated device data platforms that auto-populate CPT-compliant notes and flag threshold compliance before submission have been associated with up to 300% revenue lift through improved first-pass acceptance and the capture of previously missed billable events.
How does vendor-neutral CIED data aggregation improve accuracy over managing multiple OEM portals?
When a practice manages devices from multiple manufacturers, such as Medtronic, Boston Scientific, Abbott, and Biotronik, staff must log into separate, non-interoperable portals to retrieve each patient's transmission data. This manual process introduces transcription errors, creates data silos, and delays documentation of billable events. Each portal uses different data formats and report structures, making a consistent documentation template hard to apply across the patient population. A vendor-neutral platform that normalizes data from all OEM sources into one structured format lets practices apply a single compliant note template to every CIED patient regardless of manufacturer. This consistency matters directly for audit defense: every note contains the same required elements, including device identification, transmission timestamp, interrogation findings, arrhythmia log, clinical interpretation, and provider authentication, because the platform enforces the template at data ingestion rather than relying on manual entry. The result is a documentation workflow that scales with patient volume without scaling administrative burden.
Advisory Tags
Our automatic tagging and tracking keeps getting better - identify, manage and track multiple advisories more efficiently.
View and Acknowledge Recalls
Staff can document steps taken to resolve the recall for continuity of communication, tracking, and accountability.
Links Straight to FDA
Rhythm360 provides direct access to all the advisory details you need without additional searching and clicks.