Last updated: July 14, 2026
Cardiology practices face some of the most complex documentation and billing requirements in medicine. Remote monitoring of cardiac implantable electronic devices (CIEDs) alone uses a distinct family of CPT codes, including 93294, 93296, 93297, and 93298. Each code carries its own frequency rules, documentation thresholds, and payer-specific requirements. Physiological remote patient monitoring (RPM) adds another layer, with codes such as 99453, 99454, 99457, and 99458 that require explicit documentation of device setup, data transmission days, and time spent on treatment management.
The 2026 CPT updates further raised the bar on specificity. New codes such as 99445 for device supply covering 2–15 days and 99470 for treatment management requiring 10–19 minutes expanded the documentation details needed to bill correctly.
The financial consequences of documentation gaps are substantial. A mid-size cardiology group can lose $150,000 to $400,000 annually to preventable denials, downcoding, and missed prior authorizations. Cardiology practices without strong documentation controls commonly see first-pass claim denial rates of 15–20%, compared to the 5–8% industry benchmark, with the worst-performing practices exceeding 22%, nearly triple the healthcare average.
These elevated denial rates stem directly from a core operational challenge in CIED and RPM programs: data fragmentation. When a practice implants devices from multiple manufacturers such as Medtronic, Boston Scientific, Abbott, and Biotronik, staff must log into separate, non-interoperable OEM portals to retrieve patient data. This fragmentation creates data silos, manual transcription errors, and alert fatigue from an overwhelming volume of non-actionable notifications.
Critical events such as new-onset atrial fibrillation, ventricular tachycardia, or device malfunction can be delayed or missed entirely. The OIG added RPM fraud oversight to its 2025 Work Plan, which increases audit risk for practices whose documentation does not meet the specificity requirements CMS and commercial payers now enforce. These documentation gaps translate to the substantial annual losses mentioned above, driven by preventable denials, downcoding, and missed prior authorizations.
Rhythm360, developed by RhythmScience, is a vendor-neutral, HIPAA-compliant, cloud-based platform built for cardiology practices that manage CIEDs and chronic conditions such as heart failure and hypertension. Staff no longer need to navigate multiple OEM portals. Instead, Rhythm360 ingests and normalizes data from all major device manufacturers through API, HL7, XML, and PDF parsing that uses computer vision and AI-powered extrapolation. The result is a single, unified source of truth for every patient in the device population.
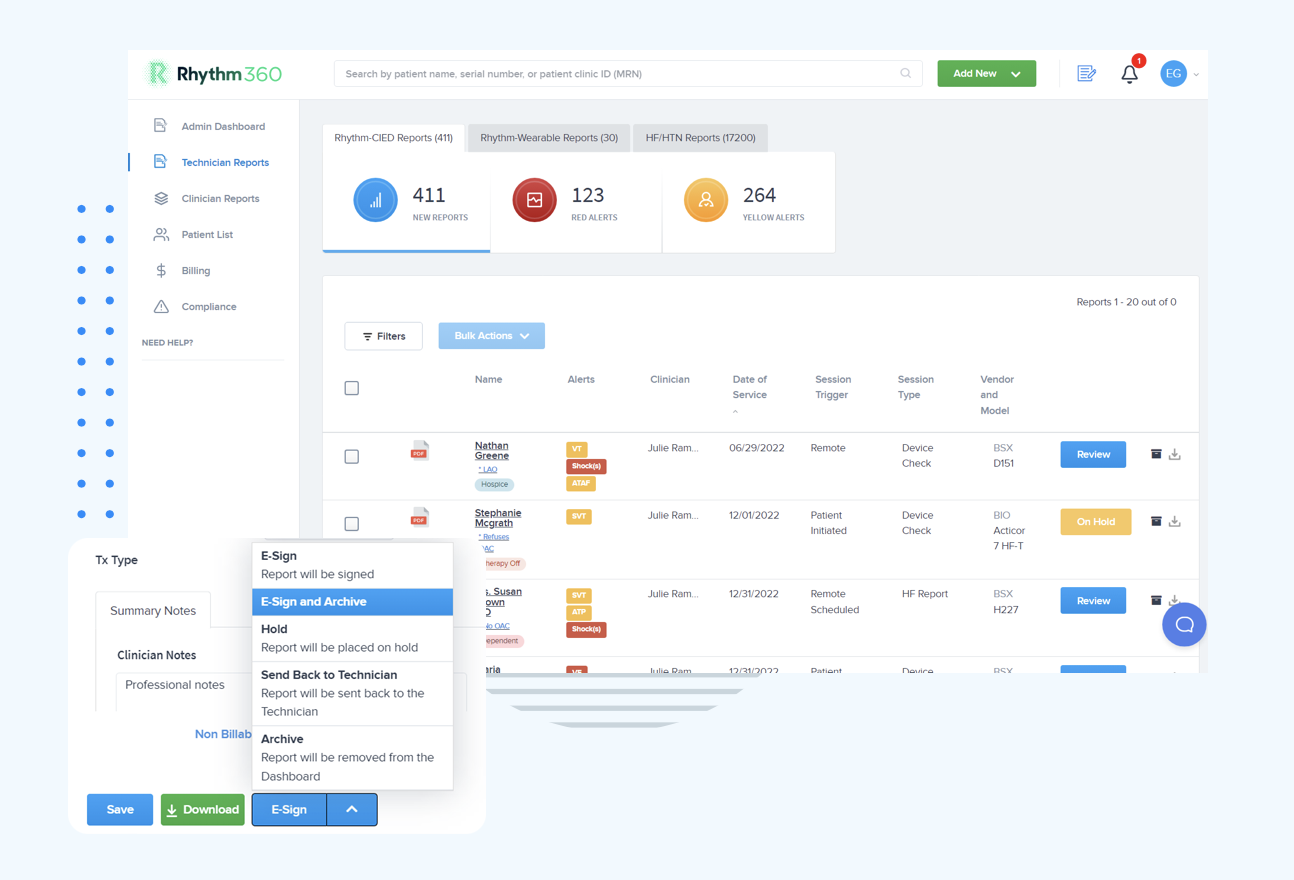
The platform’s AI-powered alert triage system filters non-actionable transmissions and surfaces clinically significant events in priority order. This directly reduces the alert fatigue that plagues manual monitoring workflows. Automated report generation, bi-directional integration with Epic, Cerner, Athenahealth, eClinicalWorks, and other EHR systems, and a secure HIPAA-compliant mobile application allow clinicians to review transmissions, sign reports, and coordinate care from any location.
These automation and AI-powered capabilities position Rhythm360 at the forefront of broader CDI industry trends. By 2026, ambient documentation has become table stakes in healthcare, with differentiation shifting to note quality by specialty, edit burden, mobile reliability, and same-day note closure rates. In cardiology, documentation must capture time-sensitive details such as arrhythmia features and device status with precision. AI-related documentation errors carry heightened clinical risk, which makes purpose-built, specialty-specific platforms the appropriate standard.
The University of Chicago Medicine used Rhythm360 to overhaul cardiovascular remote monitoring for CIED and heart failure patients. The program now manages more than 73,000 reports annually with stable dismissal rates and direct improvement in billing and accountability for patients after integration.
Rhythm360 operationalizes CDI best practices within a cardiology-specific workflow by embedding the core elements that distinguish high-performing CDI programs: real-time concurrent review, structured compliant documentation processes, data-driven prioritization, and close collaboration between clinical and coding staff.
The documentation workflow Rhythm360 enables follows a clear sequence:
The measurable outcomes of this workflow deliver the improvements noted earlier. Practices see dramatic reductions in response times and substantial revenue gains through more accurate CPT code billing. Structured CDI programs have demonstrated increases in Case Mix Index and net revenue impact, and automation plus centralization make those outcomes achievable at scale.
Demand for CDI professionals with specialty care experience continues to grow. Demand for CDI roles is growing, driven by value-based payment models and AI documentation oversight requirements. Professionals entering or advancing in the field typically follow two primary certification pathways.
CDI specialists and managers earn competitive salaries. As cardiology practices expand CIED and RPM programs, CDI specialists with remote monitoring experience, including familiarity with the 93279–93298 CIED code series and the 2026 RPM code updates, represent a particularly high-value hire.
Implementation disruption often becomes the main barrier to adopting a new clinical platform. Rhythm360 is designed to minimize that friction. The onboarding process, including EHR integration with Epic, Cerner, Athenahealth, eClinicalWorks, Greenway Health, and others via HL7, typically takes from a few days to a few weeks.
The platform’s SaaS-based pricing scales based on clinic size and usage. This structure makes Rhythm360 accessible for solo electrophysiology practices and large integrated health systems alike, without the high setup fees associated with legacy on-premise systems.
The platform also reduces dependence on a single “super-user.” By centralizing device data, alert management, and documentation into one intuitive dashboard, Rhythm360 distributes workflow across the care team. This design supports business continuity even when key staff members are unavailable.
Effective clinical documentation improvement combines concurrent review, structured physician query processes, and technology-enabled automation. Concurrent review examines records during or immediately after the clinical encounter rather than after discharge. This timing allows documentation gaps to be addressed before they affect coding and billing.
In cardiology, teams verify that remote monitoring records include specific monitoring period dates, data transmission day counts, device type, and time spent on treatment management before claims are submitted. Platforms like Rhythm360 automate data ingestion and report generation, which reduces the manual burden on clinical staff while maintaining the documentation specificity required for compliant CPT code selection. Provider education tailored to cardiology-specific requirements, such as the distinction between CIED monitoring codes and RPM physiological monitoring codes, helps sustain documentation quality over time.
The 7 C’s of clinical documentation form a framework for evaluating whether a clinical record meets the standards required for accurate coding, billing, and patient care continuity. The criteria are: Clear (unambiguous language that supports a single interpretation), Concise (relevant detail without unnecessary repetition), Complete (all diagnoses, procedures, and services documented), Consistent (no contradictions between notes, orders, and results), Correct (clinically accurate and supported by objective indicators), Contemporaneous (documented at or near the time of the encounter), and Compliant (aligned with ICD-10-CM, CPT, and payer-specific documentation requirements).
In cardiology remote monitoring, applying all seven criteria means every transmission record documents the device type, monitoring interval, data received, and clinician review, not just that monitoring occurred.
CDI specialist compensation varies by experience, credential, and care setting. According to ACDIS Salary Survey data, CDI specialists earn between $70,000 and $100,000 or more annually. CDI managers typically earn $95,000 to $130,000 or more.
Specialists with cardiology or remote monitoring experience often command a premium as practices expand CIED and RPM programs that require familiarity with complex CPT code families and 2026 code updates. Both the CCDS and CDIP certifications are associated with higher compensation and are increasingly expected by employers in specialty care environments.
The better certification depends on a candidate’s professional background and career goals. The CCDS, offered by ACDIS, is generally the preferred pathway for registered nurses transitioning into CDI roles, because it emphasizes clinical knowledge, pathophysiology, and application of that knowledge to documentation review.
The CDIP, offered by AHIMA, is generally preferred for candidates from coding or health information management backgrounds, because it places greater emphasis on ICD-10-CM or PCS coding guidelines and compliance frameworks. Both certifications require at least two years of CDI-related experience and a passing examination score.
Professionals working in cardiology CDI roles benefit from supplementing either credential with specialty-specific training on CIED monitoring codes, RPM billing requirements, and the documentation standards that support compliant claim submission in remote monitoring programs.
Fragmented device data forces manual documentation workflows, which in turn lead to incomplete CPT code capture. This cascade costs cardiology practices revenue, increases compliance exposure, and puts patient safety at risk. The solution is not simply hiring more staff. Practices need a documentation infrastructure that aggregates data automatically, surfaces critical events in real time, and generates compliant records that support accurate billing from the moment a transmission is received.
Rhythm360 by RhythmScience delivers that infrastructure. The platform unifies CIED and RPM data from all major device manufacturers into a single AI-powered, vendor-neutral environment with bi-directional EHR integration, automated report generation, and intelligent alert triage. Cardiology practices gain the documentation foundation they need to reduce denials, respond faster to critical events, and capture the revenue their clinical work has already earned.
Schedule a demo today and find out how Rhythm360 can transform clinical documentation and revenue outcomes for your cardiology practice.




