Last updated: July 14, 2026
CPT 99454 requires a patient's device to transmit readings on at least 16 separate days within a 30-day billing period. Multiple readings on the same day count as one transmission day. Manual patient data entry does not qualify. Missing the threshold means the code cannot be billed for that period, no matter how much clinical management time staff logged.
In 2026, CMS added CPT 99445 as a device-supply code for patients transmitting 2-15 days of data in a 30-day period, reimbursed at roughly the same rate as 99454. The two codes are mutually exclusive. Only one device-supply code can be billed per patient per 30-day period. Practices should still target 20 or more transmitted days a month to buffer against connectivity issues or patient non-adherence.
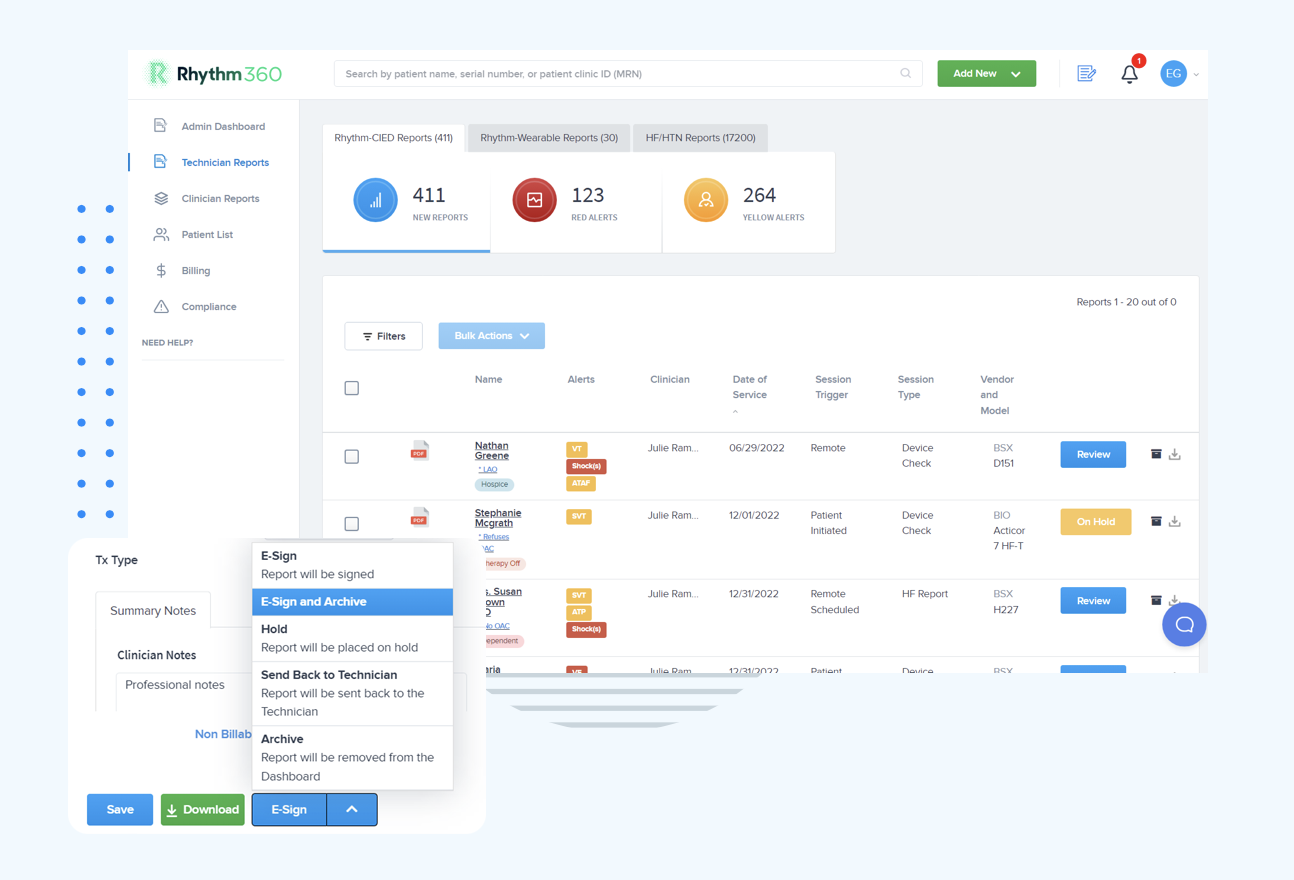
Rhythm360 ingests data from all major OEM platforms, including Medtronic, Boston Scientific, Abbott, and Biotronik, into a real-time transmission counter. Staff no longer need to log into separate portals to verify daily counts. See the threshold dashboard in action across your entire patient population.
Pro Tip: Mid-month reviews should flag patients at risk of falling below the 16-day threshold, meaning fewer than 10 transmissions by day 15. Configure automated alerts at day 10 and day 15 so staff have time to contact patients and resolve connectivity issues.
Common Mistake: The 16-day threshold is the single most common source of RPM claim denials. Practices relying on end-of-month manual counts routinely discover shortfalls too late to correct them.
Step 2: Log Clinical Time Correctly for CPT 99457 and 99458
Meeting the transmission threshold only solves half the billing equation. Clinical time documentation determines whether the management codes hold up too. CPT 99457 requires at least 20 minutes of clinical staff time in a calendar month, with one interactive communication by phone, video, or live chat. Asynchronous messaging alone does not count. CPT 99458 covers each additional 20-minute increment beyond the first 20 minutes.
CMS 2026 guidance requires that clinical staff time be documented with the date, minutes, activities performed, and whether interactive communication occurred. Vague entries such as "reviewed RPM data, 20 minutes" get flagged in audits more often now.
Rhythm360 automatically logs staff time against each patient encounter, flags the required interactive contact, and keeps a running monthly total. This removes manual spreadsheets and the risk of undercounting billable minutes.
Pro Tip: Many practices miss legitimate reimbursement because time beyond the first 20 minutes goes untracked. Confirm your platform captures every increment eligible for CPT 99458 billing.
Common Mistake: Text messages, portal messages, and voicemails do not qualify as interactive communication for CPT 99457 or the new CPT 99470. Only synchronous, real-time, two-way interactions count.
Step 3: Build an Audit-Ready Patient File
A complete audit-ready RPM patient file must contain the following seven artifacts, each supporting a different piece of audit defense:
- Written patient consent including cost-sharing acknowledgment and the right to revoke
- Physician order specifying the qualifying chronic condition and monitoring type, renewed annually
- Device assignment record with FDA clearance reference
- Monthly transmission logs showing the exact count of days with valid automatically transmitted data
- Clinical time documentation for each billing period with date, duration, activity description, and staff identity
- Interactive communication record showing date, mode, and summary of discussion and actions
- Monthly summary note documenting trends, exceptions, and the forward care plan
Rhythm360 generates and stores all of these artifacts automatically within each patient record, so they are immediately retrievable during an audit.
Pro Tip: Assemble a digital "Audit Binder" with policies and procedures, vendor contracts, device FDA documents, patient consents, sample annotated claims, internal audit reports, and meeting minutes. Designate a compliance officer as the point person for rapid auditor access, and review the binder at least every six months.
Common Mistake: Internal compliance audits should review a random 10-20% sample of RPM patient records at least quarterly, checking 16-day transmission logs and time documentation quality. Practices that skip quarterly audits often find systemic documentation gaps only after a payer audit triggers recoupment.
Step 4: Keep RPM Time Separate From CCM, RTM, and TCM
RPM management codes (99457/99458) and CCM codes (99490/99491) can be billed in the same month for the same patient, provided staff time for each service is tracked separately in the EHR. Each minute must be tagged exclusively as RPM-management or CCM-management.
RPM and RTM cannot be billed together for the same patient in the same calendar month, and this prohibition remains in effect under the CY 2026 Physician Fee Schedule. The only exception applies when the two programs monitor entirely different data types for distinct conditions, such as RPM for blood pressure and RTM for respiratory therapy adherence.
Pro Tip: Each stacked program requires its own documented consent obtained before services begin. A single generic consent covering multiple programs is not sufficient. Keep separate consent documents for RPM and CCM when running both concurrently.
Common Mistake: Compressing monthly RPM, RTM, CCM, or APCM work onto a single date of service raises both MUE unit-cap exposure and PTP code-pair collision risk. Validate each month's batch against the current quarter's MUE caps and PTP edits before submission.
Step 5: Let EHR Integration Catch What Manual Checks Miss
Manually cross-checking MUE and PTP edits every month takes time and invites errors, one reason practices lean on EHR integration to automate the verification. Bi-directional HL7/FHIR EHR integration automatically pushes RPM encounter notes, alert documentation, time logs, and monthly summary reports into the patient chart, with no IT build required from the practice. This removes manual data entry, cuts transcription errors, and enables real-time eligibility checks before claims go out.
Rhythm360 integrates bi-directionally with Epic, Cerner, Athenahealth, eClinicalWorks, Greenway Health, and other systems via HL7. Transmission data, clinical time logs, and monthly reports flow automatically into the EHR, creating one source of truth for both clinical decisions and billing compliance. Onboarding, including integration setup, typically takes a few days to a few weeks.
Pro Tip: Configure RPM platforms so audio and video encounters automatically time-stamp and flow into the EHR. This eliminates most documentation errors for clinical time logging under CPT 99457/99458.
Common Mistake: Platforms without deep EHR integration create data silos that reduce billing accuracy and claims approval rates. Practices juggling disconnected portals for Medtronic, Boston Scientific, Abbott, and Biotronik data face compounding manual entry errors that surface as denials.
Step 6: Scrub Claims Before They Ever Leave the Practice
Medicare permits only one practitioner, tied to one NPI, to bill RPM services for a patient in any 30-day period, regardless of the number of devices used. Pre-submission scrubbing must verify this single-NPI rule, confirm the 16-day threshold has been met, validate that at least one interactive communication is documented, and check that ICD-10 codes support medical necessity.
Because 20-30% of RPM claims are typically delayed or denied due to the threshold, documentation, and NPI issues covered above, getting these fundamentals right matters. Practices adopting RPM saw a 20% increase in Medicare revenue relative to matched controls, and practices that avoid the common denial triggers capture more of that gain. Rhythm360's automated claim scrubber enforces all of these checks systematically before submission.
Rhythm360 focuses specifically on unifying CIED and RPM data, automating the 16-day threshold, logging clinical time, and producing audit-ready documentation within a single vendor-neutral platform.
Common Mistake: Billing CPT 99454 without devices that automatically collect and transmit patient data, relying instead on manual entry, does not meet CMS requirements. Verify every enrolled device is FDA-cleared with automatic transmission capability before submitting device-supply codes.
Watch the claim scrubber catch errors before submission and see the monthly workflow engine in action.
Frequently Asked Questions
What is the CMS final rule for remote patient monitoring transmission requirements in 2026?
Under the CY 2026 Medicare Physician Fee Schedule Final Rule, CMS replaced the all-or-nothing 16-day transmission requirement with a two-tier structure. CPT 99454 remains the device-supply code for patients who transmit on 16 or more days within a 30-day period. As covered above, CPT 99445 serves as the lower-tier device-supply code for the 2-15 day range and stays mutually exclusive with 99454. CMS also added CPT 99470 to cover brief treatment management of 10-19 minutes per month, complementing CPT 99457 and 99458 (capped at two units per month). All management codes still require at least one real-time, synchronous, two-way interactive communication per billing month.
How do I document the required interactive communication for CPT 99457?
A compliant CPT 99457 time entry must contain the date of service, patient identifier, device type and date range of readings reviewed, the staff member's name and credentials, the communication method, a brief summary of findings and actions taken, the session duration, and the cumulative monthly time. As noted earlier, asynchronous messages, texts, portal messages, and voicemails do not satisfy this requirement. Entries like "reviewed RPM data, 20 min" without a date or staff identity get flagged during Medicare audits. Time that counts toward the threshold includes reviewing readings, adjusting the treatment plan, live communication, coordinating care with other clinicians, and related chart updates.
Can RPM and CCM be billed in the same month?
Yes. CMS permits concurrent billing of RPM (99457/99458) and CCM (99490/99491) for the same patient in the same month, as long as each program's requirements are met independently and time is tracked separately. No minute of staff time counts toward both programs at once. Separate consent documents are required for each program, and each time log must record start and stop times, activity descriptions, staff identity, and the program the time belongs to. As noted earlier, RPM and RTM cannot be billed together in the same month except when addressing entirely different conditions.
What are the most common reasons for RPM claim denials in cardiology?
The most frequent sources of RPM claim denials in cardiology practices fall into five categories:
- Failure to meet the 16-day transmission threshold for CPT 99454, the single leading cause of denial
- Insufficient clinical time documentation for CPT 99457/99458, including missing dates or vague activity descriptions
- Duplicate billing across practitioners, violating the single-NPI rule
- Overlap errors between RPM, CCM, and RTM time
- Medical necessity gaps in ICD-10 coding that fail to tie the monitored parameter to a documented condition
Automated claim scrubbing that checks all five conditions before submission remains the most reliable way to prevent these denials.
Six Steps, One Compliant Workflow
Clean RPM claim submissions in cardiology require six coordinated steps. Active daily transmission monitoring with mid-month alerts comes first, followed by timestamped clinical time logging that captures every billable minute. Audit-ready documentation gets assembled automatically at the patient level. Strict separation of RPM time from CCM and RTM activities prevents overlap denials. Bi-directional EHR integration removes manual data entry, and pre-submission claim scrubbing enforces the single-NPI rule and threshold verification before any claim gets batched.
Manual execution of any one of these steps introduces risk: missed thresholds, incomplete documentation, denied claims. Rhythm360 automates all six within a single vendor-neutral platform. It ingests data from every major OEM, tracks transmission days in real time, logs interactive clinical time, generates audit-ready artifacts, integrates bi-directionally with your EHR, and scrubs claims before submission. Practices using Rhythm360 have achieved up to an 80% reduction in critical alert response times and up to a 300% increase in revenue through optimized CPT code billing.
Talk to our team about automating your RPM workflow and see how Rhythm360 removes every manual step from your billing process.





